
Photo of the week: One of the puppies
Highlight of the week: Our weekly drive in the park nets us 22 wild dog puppies moving dens
Lowlight of the week: I tweak my shoulder again and am forced to rest it
Maximum temperature: 32 degrees Celsius
Rainfall: Not yet
Hewn out of primordial bush. By plant machinery bearing the name Velos. And so, our new, all bells and all whistles District General hospital acquires its colloquial name. Velos. Near but far. Near to the airport and not too far for those who have motorised vehicles. Far from our crowds. With no transportation infrastructure to speak of. Shanks’ pony and clever Mike excepted.
The building is stunning. Throw a stone and you can hit planes as they take off from Mfuwe International Airport. There is no question that health services in Mambwe district need a shot in the arm. The Mambwe District Hospital was opened in 2024 by President Hichilema Hakainde. First impressions are good. Stacked full of pristine kit. With a floor that you can eat your dinner off. But will this punt from UK export finance be a timely hit? Or a pricey miss?
A couple of weeks back - we are greeted by the charming medical director of Velos. He desperately needs to man his brand-new pumps. Bodies on the ground. Bums on seats. Docs in scrubs. Our predecessor is pulled away from primary care. Away from his prime duties. He goes rogue. With good intentions. He tries to fill the void. But nonetheless, he leaves primary care and his paymasters rather in the lurch. Our mission, should we accept it, is to redress the balance. We still want to bolster the blossoming, secondary care Mecca that is nicknamed Velos. And yet, we need to maintain the momentum of our push to reserve hospitals for repairs, by empowering people to choose health in the community. Accessibility is key.
We make a plan. We arrange to spend one morning a week at Velos. I will do a paediatric ward round and some teaching. Keith will work with the outpatient staff. After dropping the Kakumbi outreach team. The under 5 village clinic staff can save concerns for our return. They still get a taxi service and our expertise.
It’s Tuesday morning. Our first Velos day. The alarm goes off, as usual, at 06:00. Our normal alarm clock of baboons has become a little less reliable. It’s hit or miss whether the baboons choose to jump on our roof at 05:30. Meaning that we now have to set an alarm to reliably rouse. I am not sure which is worse. A loud crash on the roof? Or a tinny annoying tune from the phone? Seedling. Chosen from the iPhone alarm menu. I switch off the phone and fall back into doze mode. Groggy. Not fully awake yet. But a second, more insistent alarm, spoils my slumber. Shimmer. Not a loud crash. Not a gentle nudge. But the doc phone’s determined cry for help. Instantly awake now. We are needed. Can you come and see one of our clients? She has fallen from her roof tent. Her wrist is at a funny angle.
We leap into action. Crash through the gears. Dressed. Banana breakfast. No coffee. Only a 5-minute drive to camp. Yet long enough to reminisce. From September last year. You may remember our Blue Peter blog (https://free-4448611.webador.co.uk/blog/1970109_blue-peter-is-alive-and-kicking). We pull a broken wrist and splint it in the bush. Old hands. But this year, everything is different. We now have a functioning hospital. Access to X-ray. To good pain relief. Anaesthesia. A plaster technician. Gone are the good old days of manipulation in the bush.
We arrive at the camp. 15 minutes after the call. No blue light needed. But still faster than your average 999 ambulance in the UK. A single giraffe knows to give us a wide berth. Our patient, Patricia, is sat at a picnic table. Head down. In obvious agony. Her right wrist is the shape of a bent dinner fork. A Colle’s fracture for sure. We check the blood supply to the hand. All good. So, no major rush for any heroics. We listen to the story. She is helping to pack up the roof tent. Coming down the ladder. She misses the last rung and steps back. Onto a wobbly log. Falling about 1 metre. Onto her outstretched hand. Pain in the wrist. No other injuries. We give her some tramadol. Make a good job with a triangular sling, for once. And arrange her transfer and admission to the district hospital. Keith calls the boss and requests that we do an MUA this morning. A Manipulation Under Anaesthesia our code words for bone setting.
The stars align. We are due at Velos today anyway. Our first day at school. We arrange to meet Patricia and her family at the new DGH in a couple of hours.
Back home, we have breakfast. Coffee. Plan our day. No time for morning exercise. We are at the clinic in Kakumbi by 08:30. Ready to take the staff to their outreach clinic. Yesterday was Farmers Day. A national holiday. So, the weekly staff meeting is bumped to today. The morning meeting is still going on. No work gets done until the meeting has finished. The clinic is relatively quiet. No emergencies. So, we sit and wait. And wait.
I am learning to be more African. Inside, I am British. Impatient. A spring that needs to uncoil. We have work to do. Eventually the meeting finishes at 09:15. The staff pile out laughing and talking. Oblivious to our time pressures. I jolly them along. But there is only one pace today. Zambia pace. We finally hit the road at 09:30.
In reality, there is no rush. Things take a long time to tick over in hospitals. We get to the hospital at 10:00. We find our patient. Comfortable. Already x-rayed. In the process of giving consent. For an MUA. We are able to reassure Patricia and her family. Explain what will happen. Make a plan with the medical team. But we have a major obstacle to overcome. We do not have scrubs. We will not be allowed in theatre without scrubs. We cannot go into theatre wearing our outdoor clothes. We don’t need to be sterile for this procedure. After all we’ve done this kind of thing out in the bush twice already. But all of the anaesthetic kit lives in theatre. So, we need to make a plan.
We stand and scratch our chins. Finally, we are told that we can wear disposable gowns over our clothes. And some theatre crocs. Progress.
Amazingly, at 10:45, we take Patricia to theatre. Bernard is our clinical officer, trained in anaesthetics. James our physio, a bone setter ready with plaster of Paris. Elvis our radiographer. Whilst still in the building, Elvis is capable of giving us instant x-ray images in theatre. In total we have ten bodies in theatre, including the patient.
Everything goes like clockwork. Patricia drifts off to sleep. Ketamine and inhalational gases on board. Keith holds Patricia’s hand firmly. James applies an equal and opposite tractional force from Patricia’s elbow. The wrist reduces beautifully. The dinner fork again matches the set. Normal shape appears. An x-ray from Elvis confirms perfect positioning. James’ team applies plaster of Paris. The plaster sets quickly. After 5 minutes Elvis gives a second magic image. All set. Patricia is allowed to wake up. After 15 minutes of fame. Or should I say 15 minutes of drug induced torpor? Isoflurane gas now switched off. Patricia slowly rouses. Practically pain free and all set to safari again.
It's sometimes grim to be a doctor. You gravitate towards those affected by misfortune. Share their tribulations. But it is often possible to turn things around. Patricia rather got out of the wrong side of bed this morning. This was made more unfortunate by her sleeping 2 metres in the air. We reflect on the highs and the lows. Patricia will not be sleeping on top of the Land Rover for the next few days. But at least the trip can go on. For now. Pain free. Healing. Set. Patricia reaches Lusaka. But the thought of a further 4 weeks in the bush with one arm in a sling is too much for her. She chooses to fly home. However, the rest of the family carry on. With their 4-week, self-drive holiday of a lifetime. Zambia, Botswana, Namibia, South Africa.
First class care provided in South Luangwa is the great success story of Mambwe District General Hospital. We play a bit part. But the staff, skills and facilities of Velos Hospital are the headline act. A state-of-the-art facility hewn out of the bush. The UK investment in Velos appears to be a big hit.
We miss our Blue Peter days. The days when the buck stopped with us. Making do with double sided sticky backed plastic. But how amazing it is now to be able to deliver such 1st class care, deep in the bush.
We find ourselves at Velos 3 times this week. Our new DGH is not an esoteric niche. But I’m getting ahead of myself. More of this later. We dream that the Valley Doctor role will become superfluous as new services become more established in South Luangwa. But this is likely a pipe dream. For now, we are happy to support the development of both primary and secondary care in our Valley.
**Permission has been given to tell the story and show the xrays. Names have been changed.

Photo cam picture of the week: Our regular Civet comes visiting

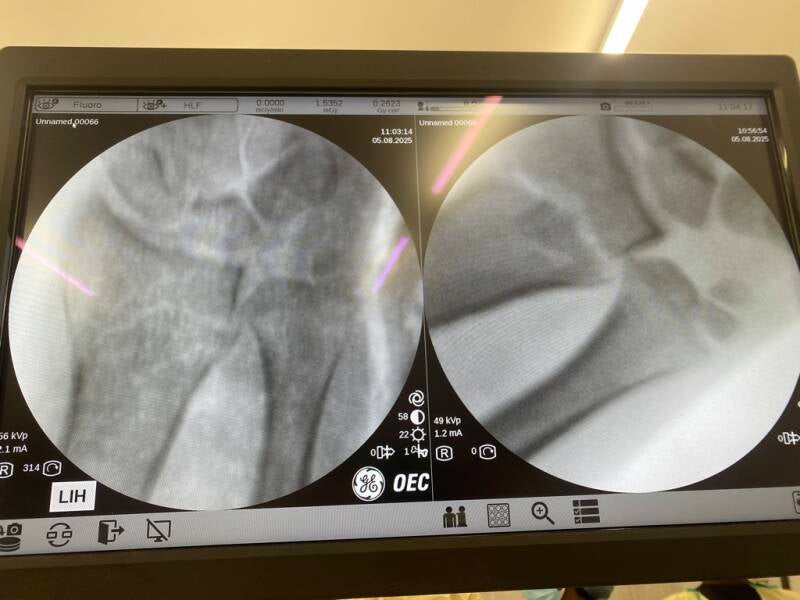

Before and after pictures. Working with Xray vision


Our team at work and when the work has finished.

Early morning giraffes.

Crocodiles see off the lion and claim the buffalo prey.
Add comment
Comments
great story and pictures- what a privilege to play such a role in helping to establish great health care :)
You wrote: We make a plan. We arrange to spend one morning a week at Velos. I will do a paediatric ward round and some teaching. Keith will work with the outpatient staff. After dropping the Kakumbi outreach team. The under 5 village clinic staff can save concerns for our return. They still get a taxi service and our expertise." Brilliant plan.
Well done you two. I really envy you the wildlife. Couldn’t do the MUA though!